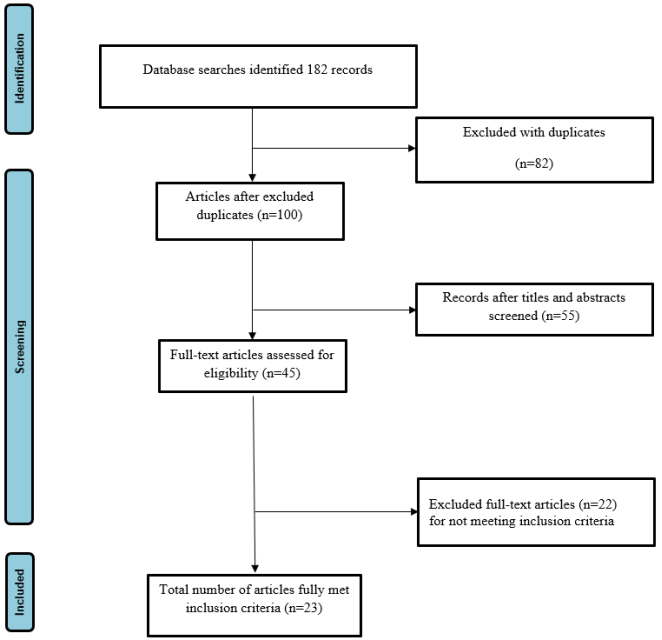
Although numerous studies have explored differences between conventional (fresh) and frozen embryo transfer in IVF/ICSI cycles, inconsistencies remain regarding their impact on neonatal outcomes. The objective of this systematic review was to comprehensively evaluate and compare pregnancy and neonatal outcomes—such as preterm birth, low birth weight, and growth parameters—between conventional embryo transfer (ET) and frozen embryo transfer (FET). A systematic literature search was conducted across major databases, including PubMed, Cochrane Library, Scopus, Web of Science, Wiley, Ovid, and ScienceDirect, covering publications from January 1980 to February 2025. Studies were included if they compared fresh and frozen embryo transfers in IVF/ICSI cycles and reported at least one neonatal or pregnancy outcome. Data extraction and quality assessment were performed independently by two reviewers using the Newcastle–Ottawa Scale (NOS) for cohort studies and the revised Cochrane Risk of Bias Tool for randomized controlled trials. Twenty-three eligible studies were identified, encompassing over 165,000 embryo transfer cycles from diverse geographic regions. The findings indicated that singleton pregnancies conceived after FET were associated with lower risks of preterm birth, low birth weight, and small-for-gestational-age infants compared to those conceived via fresh ET. Conversely, FET was linked with a higher likelihood of large-for-gestational-age and macrosomic births. RCTs and meta-analytic data further demonstrated higher clinical pregnancy and live birth rates and lower miscarriage and OHSS rates with FET. No significant differences were observed between the two groups in rates of congenital anomalies or neonatal mortality. This systematic review demonstrates that frozen embryo transfer is generally associated with more favorable neonatal outcomes than conventional fresh embryo transfer, particularly regarding fetal growth and gestational maturity. While FET offers distinct advantages, individualized treatment planning remains essential, and the decision to use fresh or frozen transfer should be based on patient characteristics and clinical context. Further prospective studies are encouraged to explore the long-term implications of both transfer methods on child health and maternal outcomes.
| Published in | Journal of Gynecology and Obstetrics (Volume 14, Issue 1) |
| DOI | 10.11648/j.jgo.20261401.11 |
| Page(s) | 1-12 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
In Vitro Fertilization, Embryo Transfer, Frozen Embryo, Pregnancy Outcome, Neonatal Health
Reference | Study design | Duration | Sample size (n) | Outcome | Risk of bias |
|---|---|---|---|---|---|
Pavlovic et al., Florida, 2024 [10] | Multicenter retrospective cohort analysis | 6 years | Fresh ET (n = 6,755) FET after freeze-all (n = 1,564) | Live birth rate was comparable between fresh ET (43.9%) and FET (45.9%) after adjusting for age, BMI, AFC, basal FSH, progesterone, peak estradiol, number of oocytes retrieved, and diagnosis. Positive pregnancy test, clinical pregnancy rate, and miscarriage rate were also comparable between fresh ET and FET across all age groups (<35, 35–37, 38–40, >40) and at different estradiol cutoffs (<4,000; 4,000–4,999; ≥5,000 pg/mL). No significant differences in CPR, miscarriage, or LBR were found across any subgroup. | Moderate risk (NOS = 7/9). Large multicenter dataset, but retrospective design and potential confounder influence. (NOS score: S ★★★★ C ★★ O ★★★) |
Cavoretto et al. Italy, 2020 [11] | Prospective cohort | 3 years | ET (n =164) FET (n =203) | Fresh ET significantly increased SGA risk (OR 4.28 [1.37–13.4]; p = 0.008). No difference for LGA or preterm birth. | (Maximum score on the NOS) Low risk (NOS = 9/9). Well-defined cohort, standardized outcomes, minimal confounding. |
Cavoretto et al. Italy, 2022 [12] | Prospective cohort | 5 years | ET (n =263) FET (n =368) | ET singletons had higher SGA (OR 2.24 [1.38–3.66]) and lower LGA (OR 0.36 [0.18–0.71]); no difference in preterm birth. | (Maximum score on the NOS) Low risk (NOS = 9/9). Large sample, clear criteria, reliable adjustment. |
Chen et al. China, 2022 [13] | Retrospective cohort | 4 years, 5 months | ET (n =375) FET (n =345) | ET was associated with a higher risk of preterm birth (OR 2.21 [1.0–4.9]; p = 0.046). No significant differences were observed for macrosomia, low birth weight (LBW), or congenital malformations between ET and FET groups. | Moderate risk (NOS = 7/9). Retrospective design; possible selection bias. (NOS score: S★★★★ C★★ O ★★★) |
Hsiao et al. Taiwan, 2023 [14] | Retrospective cohort | 12 years | ET (n =428) FET (n =356) | Singletons conceived through ET demonstrated a greater risk of preterm delivery (OR 1.54 [1.0–2.38]; p = 0.047) and low birth weight (OR 1.67 [1.05–2.66]; p = 0.028). No significant difference was reported in macrosomia, SGA, or LGA between groups. | (Maximum score on the NOS) Low risk (NOS = 8/9). Long-term data, robust methodology. |
Hwang et al. United States of America, 2019 [15] | Retrospective cohort | 9 years, 6 months | ET (n =12,390) FET (n =2101) | Infants conceived via frozen embryo transfer (FET) had higher odds of being LGA (OR 1.47 [1.26–1.7]), but lower odds of SGA (OR 0.56 [0.44–0.7]) and LBW (OR 0.72 [0.59–0.88]). There were no significant differences in preterm birth or congenital malformations between FET and ET groups. | (Maximum score on the NOS) Low risk (NOS = 9/9). Large national dataset; strong adjustment for confounders. |
Maheshwari et al. United Kingdom, 2022 [16] | Randomized controlled trial, non-blinded, parallel | 3 years, 2 months | ET (n =309) FET (n =307) | No statistically significant differences were observed between fresh (ET) and frozen embryo transfer (FET) groups in singleton pregnancies for preterm delivery, SGA, LGA, low birth weight (LBW), macrosomia, neonatal death, or congenital anomalies. The authors employed a customized approach to data reporting, presenting unadjusted risk ratios and varying confidence intervals. | Moderate risk of bias using the Cochrane Risk of Bias Tool. Randomized but non-blinded; minor reporting bias. |
Zhang et al. China, 2018 [17] | Retrospective cohort | 8 years, 2 months | ET (n =2059) FET (n =2053) | FET reduced LBW (OR 0.59 [0.37–0.98]) and SGA (OR 0.73 [0.55–0.99]) but increased LGA (OR 1.26 [1.07–1.49]) and macrosomia (OR 1.43 [1.16–1.75]). | (Maximum score on the NOS) Low risk (NOS = 8/9). Large sample; consistent reporting. |
Shavit et al. Canada, 2017 [18] | Retrospective cohort | 4 years | ET (n =575) FET (n =161) | Singletons conceived via FET demonstrated an increased risk of macrosomia (p = 0.002). However, preterm birth, SGA, LBW, and congenital malformation rates were comparable between FET and ET groups. | (Maximum score on the NOS) Moderate risk (NOS = 7/9). Small FET group; retrospective data. |
Schwarze et al. Chile, 2015 [ 19] | Retrospective cohort | 2 years | ET (n =6087) FET (n =2123) | There was no significant variation between ET and FET groups in terms of preterm delivery or low birth weight among singleton pregnancies. | (Maximum score on the NOS) Low risk (NOS = 8/9). Large sample; standardized definitions. |
Ernstad et al. Sweden, 2019 [20] | Prospective cohort | 13 years | ET (n =4469) FET (n =3650) | Transfer of vitrified blastocysts was linked to a reduced risk of LBW (OR 0.57 [0.44–0.74]) and SGA (OR 0.58 [0.44–0.78]) but an elevated risk of macrosomia (OR 1.77 [1.35–2.31]) and LGA (OR 1.48 [1.18–1.84]). No significant differences were identified in preterm birth, neonatal death, or congenital malformations. | (Maximum score on the NOS) Low risk (NOS = 9/9). National registry; long-term consistency. |
Aflatoonian et al. Iran, 2016 [21] | Prospective cohort | 4 years | ET (n =1134) FET (n =285) | No significant differences were found between groups for SGA or LBW, though FET was linked to a greater likelihood of preterm birth (OR 1.65 [1.03–2.66]; p = 0.037) in singleton pregnancies compared with ET. | (Maximum score on the NOS) Low risk (NOS = 8/9). Adequate design and reporting. |
Pereira et al. United States of America, 2016 [22] | Retrospective cohort | 3 years, 9 months | ET (n =334) FET (n =427) | Both ET and FET showed similar outcomes regarding preterm delivery and low birth weight, with no statistically significant differences observed. | (Maximum score on the NOS) Moderate risk (NOS = 6/9). Small sample and retrospective design. |
Belva et al. Belgium, 2016 [23] | Prospective cohort | 5 years | ET (n =1374) FET (n =827) | Singletons born following FET were less likely to be SGA (OR 0.55 [0.34–0.9]; p = 0.005). Other neonatal outcomes—including preterm birth, LBW, LGA, and congenital anomalies—did not differ significantly between groups. | (Maximum score on the NOS) Low risk (NOS = 9/9). Prospective design; robust data. |
Maheshwari et al. United Kingdom, 2016 [24] | Retrospective cohort | 20 years | ET (n =95,911) FET (n =16,521) | Pregnancies resulting from FET showed a lower risk of LBW but a higher risk of macrosomia compared with ET. No significant differences were reported for preterm birth or congenital malformations. The authors noted possible overlap in categories and used adjusted risk ratios with distinct confidence intervals. | (Maximum score on the NOS) Low risk (NOS = 9/9). Large national dataset; strong control for confounders. |
Kato et al. Japan, 2012 [25] | Retrospective cohort | 3 years | ET (n =2531) FET (n =4092) | Infants conceived by FET had reduced odds of SGA (OR 0.43 [0.33–0.56]) and LBW (OR 0.65 [0.53–0.79]) but showed no difference from ET in preterm birth, LGA, or congenital malformations. | (Maximum score on the NOS) Low risk (NOS = 8/9). Clear inclusion criteria; good adjustment. |
Ozgur et al. Turkey, 2015 [26] | Retrospective cohort | 2 years | ET (n =176) FET (n =116) | There were no notable differences between ET and FET groups for preterm birth or LBW outcomes. The authors reported results as risk ratios, noting slight differences in cohort composition across variables. | (Maximum score on the NOS) Moderate risk (NOS = 6/9). Small sample; limited confounder control. |
Pelkonen et al. Finland, 2010 [27] | Retrospective cohort | 11 years | ET (n =2942) FET (n =1830) | In comparison to ET, the FET group displayed lower risks of preterm birth (OR 0.83 [0.71–0.97]), LBW (OR 0.74 [0.62–0.88]), and SGA (OR 0.63 [0.49–0.83]), but a higher risk of LGA (OR 1.7 [1.21–2.40]). | (Maximum score on the NOS) Low risk (NOS = 9/9). Comprehensive national data; high validity. |
Zhang et al. China, 2020 [28] | Retrospective cohort | 6 years | ET (n =2125) FET (n =924) | Singletons conceived through FET showed a higher rate of macrosomia (OR 1.35 [1.07–1.71]; p = 0.013) but a lower risk of LBW (OR 0.67 [0.45–1.00]; p = 0.048) compared with ET. No significant differences were found for preterm birth. | Low risk (NOS = 8/9). Adequate control and reporting. (NOS score: S ★★★★ C ★★ O ★★★) |
Stormlund et al. Denmark, 2020 [29] | Randomized controlled trial, non-blinded, parallel | 2 years, 4 months | ET (n =66) FET (n =61) | Fresh single blastocyst transfer was associated with an increased risk of preterm birth (p = 0.01). There were no differences in LBW, SGA, or LGA rates between the two transfer types. | Low risk of bias using the Cochrane Risk of Bias Tool |
Aflatoonian et al. Iran, 2010 [30] | Prospective cohort | 2 years | ET (n =500) FET (n =200) | There were no statistically significant differences between ET and FET groups in preterm birth, LBW, neonatal death, or congenital malformations among singleton pregnancies. | (Maximum score on the NOS) Low risk (NOS = 8/9). Clear criteria and consistent outcomes. |
JIANG et al., China, 2023 [31] | Retrospective cohort | 6 years | Fresh ET = 313 cycles FET = 306 cycles | In fresh ET, R-ICSI embryos showed lower clinical pregnancy, implantation, and live birth rates compared with ICSI embryos. In FET cycles, there were no significant differences between R-ICSI and ICSI embryos in clinical pregnancy rate, implantation rate, ectopic pregnancy, abortion (miscarriage) rate, or live birth rate. | Moderate risk (NOS = 7/9). Retrospective single-center design; potential selection bias and limited generalizability. (NOS score: S ★★★★ C ★★ O ★★★) |
Pape et al., Switzerland, 2025 [32] | Retrospective cohort | 6 years | 2014–2016: Fresh ET (n = 1,991 women; 6,087 cycles), FET (n = 275 women; 884 cycles) | Before legislation revision, LBR was higher in fresh ET compared with FET (27.2% vs 22.7%; P = 0.006). After revision, LBR was higher in FET compared with fresh ET (36.3% vs 29.3%; P < 0.001), and cumulative LBR was higher in freeze-all cycles (59.0% vs 39.8%; P < 0.001). Multivariable mixed-model analysis showed no significant difference in live birth odds between fresh and frozen ET (OR = 1.08; 95% CI 0.95–1.22) and no superiority of freeze-all over fresh ET (IRR = 1.12; 95% CI 0.98–1.27). Fresh blastocyst transfer had higher LBR than cleavage-stage transfer (OR = 2.01; 95% CI 1.62–2.49). | Moderate risk (NOS = 7/9). Large national dataset but retrospective design; policy-period differences may influence results. (NOS score: S ★★★★ C ★★ O ★★★) |
Fattahpour et al, Iran, 2025, [33] | Prospective study | 6 years | Fresh ET (n=142); Frozen ET (n=320) | No significant differences were found in chemical pregnancy (AOR 1.31; 95% CI: 0.81–2.3), clinical pregnancy (AOR 1.51; 95% CI: 0.90–2.5), live birth rate (AOR 1.6; 95% CI: 0.54–12.4), preterm birth (AOR 0.62; 95% CI: 0.33–5.5), or primary infertility (AOR 0.73; 95% CI: 0.34–1.6) between fresh and frozen ET. The rates of chemical pregnancy (21.8% vs 17.2%), clinical pregnancy (19% vs 13.4%), and live birth (14.1% vs 9.1%) were slightly higher in fresh ET, but not statistically significant. Multiple pregnancy (5% vs 13.8%) and spontaneous abortion (22.2% vs 30.2%) were more frequent in frozen ET. | Low risk (NOS = 8/9). Representativeness of cohort, clear exposure classification, and adjusted analysis performed. Minor limitations in follow-up completeness. |
Zhang et al, China, 2018 [34] | Randomized controlled trials | Not mention | Fresh ET (n = 1141); FET (n = 1079) | FET significantly increased live birth rate (RR 1.18; 95% CI 1.08–1.30; P = 0.0003) and clinical pregnancy rate (RR 1.10; 95% CI 1.02–1.19; P = 0.02). Miscarriage rate (RR 0.62; 95% CI 0.48–0.80; P = 0.0002) and moderate–severe OHSS rate (RR 0.22; 95% CI 0.12–0.39; P < 0.00001) were significantly lower in FET. No significant differences were found for biochemical pregnancy, ongoing pregnancy, or implantation rates. | Low risk (NOS = 9/9). High-quality RCTs included; comprehensive search strategy; consistent effect estimates; low heterogeneity for major outcomes. |
Coates et al., United States, 2017 [35] | Randomized controlled trial | 1 year 8 months | Fresh ET (n= 88); Frozen ET (n= 91) | Implantation rate per embryo transferred was slightly higher in the frozen group compared with fresh ET (75% vs. 67%; not statistically significant). Ongoing pregnancy rate (80% vs. 61%) and live birth rate per ET (77% vs. 59%) were significantly higher in the frozen group. | Low risk (NOS = 9/9). Randomization performed, well-defined population, standardized outcome measures, minimal risk of bias. |
AFC | Antral Follicle Count |
AOR | Adjusted Odds Ratio |
ART | Assisted Reproductive Technology |
BMI | Body Mass Index |
CI | Confidence Interval |
CPR | Clinical Pregnancy Rate |
DPI | Dry Powder Inhaler |
ET | Embryo Transfer |
FET | Frozen Embryo Transfer |
FSH | Follicle-stimulating Hormone |
GnRH | Gonadotropin-releasing Hormone |
HRT | Hormone Replacement Therapy |
ICSI | Intracytoplasmic Sperm Injection |
IRR | Incidence Rate Ratio |
IVF | In Vitro Fertilization |
LBW | Low Birth Weight |
LBR | Live Birth Rate |
LGA | Large for Gestational Age |
MeSH | Medical Subject Headings |
NOS | Newcastle–Ottawa Scale |
OHSS | Ovarian Hyperstimulation Syndrome |
OR | Odds Ratio |
PCOS | Polycystic Ovary Syndrome |
PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
RCT | Randomized Controlled Trial |
RoB 2 | Revised Cochrane Risk of Bias Tool (Version 2) |
RR | Risk Ratio |
R-ICSI | Rescue Intracytoplasmic Sperm Injection |
SD | Standard Deviation |
SGA | Small for Gestational Age |
| [1] | Bentov Y, Schenker J. IVF and pregnancy outcomes: the triumphs, challenges, and unanswered questions. J Ovarian Res. 2025; 18(1): 228. |
| [2] | Zhang Q, Chen Q, Li T, Jia Z, Bu X, Liu Y, et al. Pregnancy outcomes of freeze-all versus fresh embryo transfer in women with adenomyosis: a retrospective study. J Clin Med. 2023; 12(5): 1740. |
| [3] | Roque M, Haahr T, Geber S, Esteves SC, Humaidan P. Fresh versus elective frozen embryo transfer in IVF/ICSI cycles: a systematic review and meta-analysis of reproductive outcomes. Hum Reprod Update. 2019; 25(1): 2–14. |
| [4] | Roelens C, Blockeel C. Impact of different endometrial preparation protocols before frozen embryo transfer on pregnancy outcomes: a review. Fertil Steril. 2022; 118(5): 820–827. |
| [5] | Bourdon M, Santulli P, Maignien C, Bordonne C, Millischer AE, Chargui A, et al. The “freeze-all” strategy seems to improve the chances of birth in adenomyosis-affected women. Fertil Steril. 2024; 121(3): 460–469. |
| [6] | Elhelw EM, El Serour AG, Rady MS, Abdeltawab A. Freeze-all policy versus luteal phase support with low-dose hCG in high-responder ICSI patients. Middle East Fertil Soc J. 2022; 27(1): 20. |
| [7] | Wei D, Sun Y, Zhao H, Yan J, Zhou H, Gong F, et al. Frozen versus fresh embryo transfer in women with low prognosis for IVF: pragmatic multicentre RCT. BMJ. 2025; 388. |
| [8] | Petersen SH, Westvik-Johari K, Spangmose AL, Pinborg A, Romundstad LB, Bergh C, et al. Risk of hypertensive disorders of pregnancy after fresh and frozen embryo transfer. Hypertension. 2023; 80(2): e6–e16. |
| [9] | Borji A, Haick H, Pohn B, Graf A, Zakall J, Islam SM, et al. An integrated optimization and deep learning pipeline for predicting live birth success in IVF using feature optimization and transformer-based models. 2024 Dec 27. |
| [10] | Pavlovic ZJ, Smotrich GE, New EP, Jahandideh S, Devine K, Imudia AN, et al. Fresh vs frozen: pregnancy outcomes and treatment efficacy. F&S Rep. 2024; 5(4): 369–377. |
| [11] | Cavoretto PI, Farina A, Gaeta G, Sigismondi C, Spinillo S, Casiero D, et al. Uterine artery Doppler in singleton IVF pregnancies after fresh vs frozen blastocyst transfer. Ultrasound Obstet Gynecol. 2020; 56: 603–610. |
| [12] | Cavoretto PI, Farina A, Gaeta G, Seidenari A, Pozzoni M, Spinillo S, et al. Greater fetal and birth weight after frozen vs fresh blastocyst transfer. Ultrasound Obstet Gynecol. 2022; 60: 76–85. |
| [13] | Chen Y, Zhou J, Chen Y, Yang J, Hao Y, Feng T, et al. Pregnancy outcomes after frozen and fresh embryo transfer in advanced maternal age. J Clin Med. 2022; 11: 6395. |
| [14] | Hsiao YY, Chen CM, Chen YC, Tsai NC, Su YT, Li YL, et al. Birth outcomes after frozen vs fresh embryo transfer in Taiwan. J Obstet Gynaecol. 2023; 62: 59–65. |
| [15] | Hwang SS, Dukhovny D, Gopal D, Cabral H, Diop H, Coddington CC, et al. Health outcomes after fresh versus frozen embryo transfer. Fertil Steril. 2019; 112: 900–907. |
| [16] | Maheshwari A, Bari V, Bell JL, Bhattacharya S, Bhide P, Bowler U, et al. Thawed frozen versus fresh embryo transfer (E-Freeze RCT). Health Technol Assess. 2022; 26: 1–142. |
| [17] | Zhang J, Du M, Li Z, Wang L, Hu J, Zhao B, et al. Fresh versus frozen embryo transfer for singleton birth. J Ovarian Res. 2018; 11: 59. |
| [18] | Shavit T, Oron G, Weon-Young S, Holzer H, Tulandi T. Maternal complications after vitrified-warmed single-embryo transfer. Reprod Biomed Online. 2017; 35: 94–102. |
| [19] | Schwarze JE, Crosby JA, Zegers-Hochschild F. Effect of embryo freezing on perinatal outcome. Reprod Biomed Online. 2015; 31: 39–43. |
| [20] | Ernstad EG, Spangmose AL, Opdahl S, Henningsen AK, Romundstad LB, Tiitinen A, et al. Perinatal outcomes after vitrified blastocyst transfer. Hum Reprod. 2019; 34: 2282–2289. |
| [21] | Aflatoonian A, Karimzadeh Maybodi MA, Aflatoonian N, Tabibnejad N, Amir-Arjmand MH, Soleimani M, et al. Perinatal outcomes after fresh versus frozen embryo transfer. Int J Reprod Biomed. 2016; 14: 167–172. |
| [22] | Pereira N, Petrini AC, Lekovich JP, Schattman GL, Rosenwaks Z. Perinatal outcomes after fresh and frozen-thawed blastocyst transfer. Int J Gynaecol Obstet. 2016; 135: 96–100. |
| [23] | Belva F, Bonduelle M, Roelants M, Verheyen G, Van Landuyt L. Neonatal health including congenital malformation risk of 1072 children born after vitrified embryo transfer. Hum Reprod. 2016; 31: 1610–1620. |
| [24] | Maheshwari A, Raja EA, Bhattacharya S. Obstetric outcomes after fresh or frozen embryo transfer. Fertil Steril. 2016; 106: 1703–1708. |
| [25] | Kato O, Kawasaki N, Bodri D, Kuroda T, Kawachiya S, Kato K, et al. Neonatal outcomes after vitrified versus fresh single-embryo transfer. Eur J Obstet Gynecol Reprod Biol. 2012; 161: 46–50. |
| [26] | Ozgur K, Berkkanoglu M, Bulut H, Humaidan P, Coetzee K. Perinatal outcomes after vitrified-warmed blastocyst transfer. Fertil Steril. 2015; 104: 899–907.e3. |
| [27] | Pelkonen S, Koivunen R, Gissler M, Nuojua-Huttunen S, Suikkari AM, Hydén-Granskog C, et al. Perinatal outcome after frozen and fresh embryo transfer. Hum Reprod. 2010; 25: 914–923. |
| [28] | Zhang X, Bai L, Ren H, Liu X, Guo S, Xu P, et al. Outcomes after frozen versus fresh embryo transfer in advanced maternal age. Eur J Obstet Gynecol Reprod Biol. 2021; 257: 133–137. |
| [29] | Stormlund S, Sopa N, Zedeler A, Bogstad J, Prætorius L, Nielsen HS, et al. Freeze-all versus fresh blastocyst transfer. BMJ. 2020; 370: m2519. |
| [30] | Aflatoonian A, Mansoori Moghaddam F, Mashayekhy M, Mohamadian F. Early pregnancy and neonatal outcomes after frozen vs fresh embryo transfer. J Assist Reprod Genet. 2010; 27: 695–700. |
| [31] | Jiang Y, Yuan JC, Song G, Zhang XH, Miao SB, Wu XH. Comparing pregnancy outcomes after early rescue ICSI. |
| [32] | Pape J, Levy J, Makieva S, von Wolff M. Legal framework and IVF outcomes in Switzerland. Reprod Biomed Online. 2025; 50(2): 104483. |
| [33] | Fattahpour SF, Hakimi P, Tabatabaei F, Hejazad M, Amoozadeh M, Sadeghi L, et al. Live birth and fetal outcomes after fresh vs frozen embryo transfer. BMC Pregnancy Childbirth. 2025; 25: 122. |
| [34] | Zhang W, Xiao X, Zhang J, Wang W, Wu J, Peng L, Wang X. Frozen versus fresh embryo transfer: meta-analysis of RCTs. Arch Gynecol Obstet. 2018; 298: 259–272. |
| [35] | Coates A, Kung A, Mounts E, Hesla J, Bankowski B, Barbieri E, et al. Fresh versus frozen euploid embryo transfer. Fertil Steril. 2017; 107: 723–730. |
| [36] | European Society of Human Reproduction and Embryology (ESHRE). Factsheets and infographics. 2024. 2024 (cit-ed 2024 Jun 1). Available from: |
| [37] |
Cochrane Training. RevMan software. 2024. (cited 2024 Jun 1). Available from:
https://training.cochrane.org/online-learning/core-software/revman |
| [38] | Alpha Scientists in Reproductive Medicine; ESHRE SIG of Embryology. Istanbul consensus on embryo assessment. Hum Reprod. 2011; 26: 1270–1283. |
| [39] | Zaat T, Zagers M, Mol F, Goddijn M, van Wely M, Mastenbroek S. Fresh versus frozen embryo transfers. Cochrane Database Syst Rev. 2021; (2). |
| [40] | Higgins JPT, Thomas J, Chandler J, et al., editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5. 2024. Cochrane; 2024 (cited 2024 Jun 1). Available from: |
APA Style
Munira, S., Khanam, S. M., Akter, S. (2026). Conventional Versus Frozen Embryo Transfer in IVF/ICSI Cycles: A Systematic Review of Pregnancy Outcome. Journal of Gynecology and Obstetrics, 14(1), 1-12. https://doi.org/10.11648/j.jgo.20261401.11
ACS Style
Munira, S.; Khanam, S. M.; Akter, S. Conventional Versus Frozen Embryo Transfer in IVF/ICSI Cycles: A Systematic Review of Pregnancy Outcome. J. Gynecol. Obstet. 2026, 14(1), 1-12. doi: 10.11648/j.jgo.20261401.11
@article{10.11648/j.jgo.20261401.11,
author = {Serajoom Munira and Sadia Mahfiza Khanam and Sumaiya Akter},
title = {Conventional Versus Frozen Embryo Transfer in IVF/ICSI Cycles: A Systematic Review of Pregnancy Outcome},
journal = {Journal of Gynecology and Obstetrics},
volume = {14},
number = {1},
pages = {1-12},
doi = {10.11648/j.jgo.20261401.11},
url = {https://doi.org/10.11648/j.jgo.20261401.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20261401.11},
abstract = {Although numerous studies have explored differences between conventional (fresh) and frozen embryo transfer in IVF/ICSI cycles, inconsistencies remain regarding their impact on neonatal outcomes. The objective of this systematic review was to comprehensively evaluate and compare pregnancy and neonatal outcomes—such as preterm birth, low birth weight, and growth parameters—between conventional embryo transfer (ET) and frozen embryo transfer (FET). A systematic literature search was conducted across major databases, including PubMed, Cochrane Library, Scopus, Web of Science, Wiley, Ovid, and ScienceDirect, covering publications from January 1980 to February 2025. Studies were included if they compared fresh and frozen embryo transfers in IVF/ICSI cycles and reported at least one neonatal or pregnancy outcome. Data extraction and quality assessment were performed independently by two reviewers using the Newcastle–Ottawa Scale (NOS) for cohort studies and the revised Cochrane Risk of Bias Tool for randomized controlled trials. Twenty-three eligible studies were identified, encompassing over 165,000 embryo transfer cycles from diverse geographic regions. The findings indicated that singleton pregnancies conceived after FET were associated with lower risks of preterm birth, low birth weight, and small-for-gestational-age infants compared to those conceived via fresh ET. Conversely, FET was linked with a higher likelihood of large-for-gestational-age and macrosomic births. RCTs and meta-analytic data further demonstrated higher clinical pregnancy and live birth rates and lower miscarriage and OHSS rates with FET. No significant differences were observed between the two groups in rates of congenital anomalies or neonatal mortality. This systematic review demonstrates that frozen embryo transfer is generally associated with more favorable neonatal outcomes than conventional fresh embryo transfer, particularly regarding fetal growth and gestational maturity. While FET offers distinct advantages, individualized treatment planning remains essential, and the decision to use fresh or frozen transfer should be based on patient characteristics and clinical context. Further prospective studies are encouraged to explore the long-term implications of both transfer methods on child health and maternal outcomes.},
year = {2026}
}
TY - JOUR T1 - Conventional Versus Frozen Embryo Transfer in IVF/ICSI Cycles: A Systematic Review of Pregnancy Outcome AU - Serajoom Munira AU - Sadia Mahfiza Khanam AU - Sumaiya Akter Y1 - 2026/01/19 PY - 2026 N1 - https://doi.org/10.11648/j.jgo.20261401.11 DO - 10.11648/j.jgo.20261401.11 T2 - Journal of Gynecology and Obstetrics JF - Journal of Gynecology and Obstetrics JO - Journal of Gynecology and Obstetrics SP - 1 EP - 12 PB - Science Publishing Group SN - 2376-7820 UR - https://doi.org/10.11648/j.jgo.20261401.11 AB - Although numerous studies have explored differences between conventional (fresh) and frozen embryo transfer in IVF/ICSI cycles, inconsistencies remain regarding their impact on neonatal outcomes. The objective of this systematic review was to comprehensively evaluate and compare pregnancy and neonatal outcomes—such as preterm birth, low birth weight, and growth parameters—between conventional embryo transfer (ET) and frozen embryo transfer (FET). A systematic literature search was conducted across major databases, including PubMed, Cochrane Library, Scopus, Web of Science, Wiley, Ovid, and ScienceDirect, covering publications from January 1980 to February 2025. Studies were included if they compared fresh and frozen embryo transfers in IVF/ICSI cycles and reported at least one neonatal or pregnancy outcome. Data extraction and quality assessment were performed independently by two reviewers using the Newcastle–Ottawa Scale (NOS) for cohort studies and the revised Cochrane Risk of Bias Tool for randomized controlled trials. Twenty-three eligible studies were identified, encompassing over 165,000 embryo transfer cycles from diverse geographic regions. The findings indicated that singleton pregnancies conceived after FET were associated with lower risks of preterm birth, low birth weight, and small-for-gestational-age infants compared to those conceived via fresh ET. Conversely, FET was linked with a higher likelihood of large-for-gestational-age and macrosomic births. RCTs and meta-analytic data further demonstrated higher clinical pregnancy and live birth rates and lower miscarriage and OHSS rates with FET. No significant differences were observed between the two groups in rates of congenital anomalies or neonatal mortality. This systematic review demonstrates that frozen embryo transfer is generally associated with more favorable neonatal outcomes than conventional fresh embryo transfer, particularly regarding fetal growth and gestational maturity. While FET offers distinct advantages, individualized treatment planning remains essential, and the decision to use fresh or frozen transfer should be based on patient characteristics and clinical context. Further prospective studies are encouraged to explore the long-term implications of both transfer methods on child health and maternal outcomes. VL - 14 IS - 1 ER -
Department of Reproductive Endocrinology and Infertility, DNCC Dedicated COVID-19 Hospital, Dhaka, Bangladesh
Department of Obstetrics and Gynaecology, Dhaka Medical College Hospital, Dhaka, Bangladesh
Department of Reproductive Endocrinology and Infertility, IVF Centre, Dhaka, Bangladesh